Скачать с ютуб Acute Coronary Syndrome: What You Need To Know в хорошем качестве
Acute Coronary Syndrome: What You Need To Know
1 год назад
Скачать бесплатно Acute Coronary Syndrome: What You Need To Know в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно Acute Coronary Syndrome: What You Need To Know или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон Acute Coronary Syndrome: What You Need To Know в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
Acute Coronary Syndrome: What You Need To Know
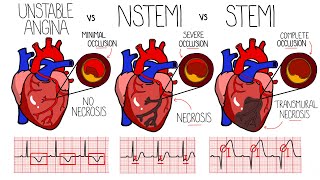
. Chapters 0:00 Introduction 0:46 Types of Acute Coronary Syndrome 1:27 Causes of Acute Coronary Syndrome 2:05 Symptoms of Acute Coronary Syndrome 2:46 Treatment for Acute Coronary Syndrome Acute coronary syndrome (ACS) is a syndrome (a set of signs and symptoms) due to decreased blood flow in the coronary arteries such that part of the heart muscle is unable to function properly or dies.[1] The most common symptom is centrally located chest pain, often radiating to the left shoulder[2] or angle of the jaw, crushing, central and associated with nausea and sweating. Many people with acute coronary syndromes present with symptoms other than chest pain, particularly women, older people, and people with diabetes mellitus.[3] Acute coronary syndrome is subdivided in three scenarios depending on the duration of symptoms, the presence of ECG changes and blood test results:[4] ST elevation myocardial infarction (STEMI, 30%), non-ST elevation myocardial infarction (NSTEMI, 25%), or unstable angina (38%).[5] Generally, when symptoms occur for less than 30 minutes, it is unstable angina. When symptoms are prolonged for more than 30 minutes, the diagnosis is acute myocardial infarction.[6] ACS should be distinguished from stable angina, which develops during physical activity or stress and resolves at rest. In contrast with stable angina, unstable angina occurs suddenly, often at rest or with minimal exertion, or at lesser degrees of exertion than the individual's previous angina ("crescendo angina"). New-onset angina is also considered unstable angina, since it suggests a new problem in a coronary artery. The cardinal symptom of critically decreased blood flow to the heart is chest pain, experienced as tightness around or over the chest and (often, but not always) radiating to the left arm and the left angle of the jaw. This may be associated with diaphoresis (sweating), nausea and vomiting, as well as shortness of breath. In many cases, the sensation is "atypical", with pain experienced in different ways or even being completely absent (which is more likely in female patients and those with diabetes). Some may report palpitations, anxiety or a sense of impending doom (angor animi) and a feeling of being acutely ill. The description of the chest discomfort as a pressure has little utility in aiding a diagnosis as it is not specific for ACS.[7] Though ACS is usually associated with coronary thrombosis, it can also be associated with cocaine use.[8] Chest pain with features characteristic of cardiac origin (angina) can also be precipitated by profound anemia, brady- or tachycardia (excessively slow or rapid heart rate), low or high blood pressure, severe aortic valve stenosis (narrowing of the valve at the beginning of the aorta), pulmonary artery hypertension and a number of other conditions.[9] Pathophysiology In those who have ACS, atheroma rupture is most commonly found 60% when compared to atheroma erosion (30%), thus causes the formation of thrombus which block the coronary arteries. Plaque rupture is responsible for 60% in ST elevated myocardial infarction (STEMI) while plaque erosion is responsible for 30% of the STEMI and vice versa for Non ST elevated myocardial infarction (NSTEMI). In plaque rupture, the content of the plaque are lipid rich, collagen poor, with abundant inflammation which is macrophage predominant, and covered with a thin fibrous cap. Meanwhile, in plaque erosion, the plaque is rich with extracellular matrix, proteoglycan, glycoaminoglycan, but without fibrous caps, no inflammatory cells, and no large lipid core. After the coronary arteries are unblocked, there is a risk of reperfusion injury due spreading inflammatory mediators throughout the body. Investigations is still underway on the role of Cyclophilin D in reducing the reperfusion injury.[10] Other, less common, causes of acute coronary syndrome include spontaneous coronary artery dissection [11] and myocardial infarction in the absence of obstructive coronary artery disease (MINOCA).[12]
Comments