Скачать с ютуб SIADH for USMLE Step 1 and USMLE Step 2 в хорошем качестве
SIADH for USMLE Step 1 and USMLE Step 2
7 лет назад
Скачать бесплатно SIADH for USMLE Step 1 and USMLE Step 2 в качестве 4к (2к / 1080p)
У нас вы можете посмотреть бесплатно SIADH for USMLE Step 1 and USMLE Step 2 или скачать в максимальном доступном качестве, которое было загружено на ютуб. Для скачивания выберите вариант из формы ниже:
Загрузить музыку / рингтон SIADH for USMLE Step 1 and USMLE Step 2 в формате MP3:
Если кнопки скачивания не
загрузились
НАЖМИТЕ ЗДЕСЬ или обновите страницу
Если возникают проблемы со скачиванием, пожалуйста напишите в поддержку по адресу внизу
страницы.
Спасибо за использование сервиса savevideohd.ru
SIADH for USMLE Step 1 and USMLE Step 2
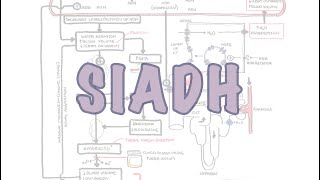
Handwritten video lecture on pathogenesis, pathophysiology symptoms and treatment of SIADH for USMLE Step 1 and USMLE Step 3. In SIADH there is increased secretion of ADH or vasopressin which leads to increase reabsorption of water leading to water intoxication. PHYSIOLOGY OF ADH Osmoreceptors detect high osmolality which activates the hypothalamus to produce and release ADH. ADH is then stored in the posterior pituitary and released. Once released ADH activates the V1 receptor which leads to vasoconstriction. ADH also activates V2 receptor in the collecting ducts which contain the principal cells. ADH enters the cells and activates vesicles which are lined with aquaporin 2 channels. This leads to increased reabsorption of water through the aquaporin channel due to high osmolality in medulla. PATHOGENESIS AND PATHOPHYSIOLOGY OF SIADH Patient is ingesting water however not able to suppress ADH and there is water retention. Increase in extracellular fluid volume which activates secondary naturietic mechanisms such as increasing ANP and Decreasing RAAS. This is able to restore the blood volume in SIADH patients, but there is a loss of sodium leading to hyponatremia. SIGNS AND SYMPTOMS OF SIADH Symptoms primarily associated with hyponatremia. Neurological symptoms such as malaise, coma, obtundation. Patients with SIADH will have low plasma osmolality, hyponatremia, high urine osmolality. Also remember in SIADH the potassium will be normal because of cellular shift that my occur. ETIOLOGY OF SIADH CNS Causes of SIADH include Stroke, hemorrhage, infections, trauma. Subarachnoid hemorrhage can also lead to cerebral salt wasting as well as SIADH. In both cases ADH will be high but in cerebral salt wasting it will be high secondarily to loss of salt. Drugs associated with SIADH include carbamazepine, chlorpropramide, cyclophosphamide, SSRI, desmopressin, oxytocin. Tumor associated with SIADH are small cell lung cancer, head and neck tumors, olfactory neuroblastoma. Many pulmonary conditions may also lead to SIADH including pneumonia, asthma, ARDS, atelectasis. Surgery of the pituitary can lead to SIADH. Endocrine abnormalities such as hypothyroidism may be a cause of SIADH. Hereditary conditions of SIADH include V2 receptor mutation. TREATMENT OF SIADH Treat any underlying cause or discontinue medication causing SIADH which will usually reverse SIADH. Correct sodium slowly (less than 9meq/L within 24 hours) or it may lead to osmotic demyelination. Fluid restriction of less than 800ml/day this can start to increase serum sodium. But don’t use fluid restriction in patients with subarachnoid hemorrhage. Hypertonic saline IV to replace sodium as they lose water. Still continues to activate ANP and decrease RAAS but can be afforded because of increase sodium. Increase solute intake to help replenish the sodium loss. May consider loop diuretic if urine osmolality is greater than 500mosmols. Vasopressin antagonist such as tolvaptan and conivaptan are also useful in SIADH. Demeclocycline and lithium both block the function of ADH and there are useful in SIADH.
Comments